I have been noticeably short of breath since getting a pretty bad case of Covid (hospitalized), and that was months ago.
Even things like climbing stairs has become a chore. One top of that, I was experiencing syncope on standing which they sent me to a cardiologist for. I couldn't complete the treadmill test to anyone's satisfaction so now we have to explore this further.
None of this existed prior to getting Covid, and it's far past the point of "it's all in my head". With the fainting on standing, I would literally drop to my knees as the world faded to black. I've never experienced anything like that in my life.
The shortness of breath is just another one to add to a list of problems now.
Note I was double-vaxxed when I caught Covid. I'll have to assume Omnicron although I have no actual data on that. It was a breakthrough case and I had a 104 fever, cough, and shortness of breath (that's why they admitted me). It's been downhill since then.
I wrote the date and times of activities that drained me - and the recovery time of rest before I felt average.
This included phone conversations, which I found had about a 14 minute limit.
It was helpful in communicating with other health professionals a little, but immensely helpful in seeing a couple weeks go by and my activities got longer / further, and the recovery time got shorter.
This also helped with the feelings of dread and worry when in the middle of something, I felt complete exhaustion - knowing I could look at a clock and count on 2 minutes to go by and I would be mostly normal again..
Things like that had a huge impact for me.
After some months, looking back on where things were, I feel that I am doing okay, and better than I was, even if I am not where I'd like to be.
I had a bad case of pneumonia that put me in the hospital for a couple days a few years back (early 30s at the time) - and it was year plus before my lungs were back to "normal"... I'm asthmatic so even my normal isn't that great. Was having to do nebulizer treatments basically every day for months.
Interesting. I didn't get hospitalized but I had what appeared to have been covid in April 2020. Before that I was running 10k quite happily but couldn't manage round the park for 2 months afterwards even though I just had a temperature and fatigue for a couple of weeks as symptoms. It took me 9 months to get over it completely.
Mostly walking to start with and practicing breathing deeply and properly when doing it. This got faster and longer and I slowly pushed it daily. Then I started going hiking again after about 5 months. Then started running again after that. I have an Apple Watch which does a reasonable approximation of cardio fitness under VO2 so I could monitor progress.
I'm no exercise expert but what appears to be important is keeping your heart rate above 120bpm for long periods of time.
2 years down the line I can do 40k walk / hilly hike without even being bothered. But I still have trouble doing a 10k run. 5k is doable easily.
> I'm no exercise expert but what appears to be important is keeping your heart rate above 120bpm for long periods of time.
Well, post-COVID that was happening without exercise. Fortunately, things went back to normal over time, my student insurance sends us to the "student health center" and they were convinced 120 was a normal resting heart rate for an otherwise healthy 26 y.o. who was used to half that a year before.
I know what that is like. About 3 years ago I started running. I need to do something, anything, as sitting at a desk all day is not healthy. I did no sport and was mildly overweight and getting heavier. I'm was in my mid 40s and it was kinda getting important to get fit.
Running is cheap and can be done any time I have time. So I started. I had to have music to make it not boring (still do but now mostly listen to podcasts).
I hated running but disliked being unfit more. Started with 2k and walked some of it. I made a big effort to go out and do it whenever I had time, 3 times a week. I can't stress this enough, but how far and fast I ran was not nearly as important as getting in the habit. Even if it was cold or a little wet. Building the habit is the only important thing for the first 6 months. Even on holidays I would bring my shoes and shorts. After a couple of months 5k was easy. I bought a heart rate monitor as a reward for getting to 5k. This was brilliant! I started getting self competitive and learned that running at a speed which kept my heart rate under 140 was the best for training. Slowly over the next two years I was able to do longer and longer distances, lost weight, slept better and found running very enjoyable and a great de-stresser. Time for myself away from the usual pressure of life and it was good for me. I enjoyed discovering the place in a new way. I got to half marathons once a month. I couldn't really believe it. Signed up for a marathon and while training for that was actually hard work and the marathon itself was crazy hard, I managed it under 4h.
Now this isn't a "look at me I'm great" story. The point is someone who couldn't run 5k at all can actually over a modest number of years get to marathon shape and enjoy it. Anyone (who doesn't have some condition) can do it. Running 5k three times a week is exceedingly good for your health and mental well being.
The key for me at least is habit. Getting into the habit is the only truly hard thing. When it's cold, windy, whatever, get out there for at least 5 minutes.
Yep, I built up to 5k right before the pandemic then stopped back when we had no damn idea how it all spread.
Just turned 50 and I built up to doing 5k every other day and I've been doing that consistently now for over 2 months.
Its gotten easier, I'm dragging ass in patches now rather than most of the second half.
Doubt I'm going to start marathoning, I'm going to try to stick to 5k for life more or less. I know eventually I'll want to push up to 8k to 10k occasionally to get my 5k times up. But generally I don't want much more than a 30 minute per day commitment.
And I started in the middle of winter in Seattle, so I've already run through all the wet and cold and windy. Could have used my scuba diving gear a few times...
Haha that feeling of running in awful weather and knowing, "well it can't get worse!" :)
And honestly the marathons and even half marathons are not important, imo. Getting over 10k regularly was very nice though. It's a different mental state at those distances.
I am not in your case, but after years of crashed cardiovascular capacity, 6 months of regular bike plus a bit of upper body workout finally brought back some sense of normalcy in my breathing. Just the sense of having some room for air inside your chest. Anyway I hope you can find a rehab plan to help you get back up. And support and patience.
ps: cardio and lung go together, so don't forget to let your heart rise up to ensure good blood flow and blood pressure, it will help your lungs too. Taichi or yoga like poses (and walking) are wonder to bootstrap blood flow in weak health.
> Just the sense of having some room for air inside your chest.
Thanks this is exactly what I need.
It's so surreal to just have a slightly long sentence in front of a group of people, only to end up catching your breath, to realize how vitally important this all is.
yes, it's partly debilitating and a strange realization
i should add, anxiety level can influence this system a lot, and when you start to have issue (covid context not helping) it might also play a role. i'm no doctor again, but i've read that capillaries have microscopic valve on both ends to control blood flow, anxiety -> nervous system -> shut capillaries.. so even if you try to breath, oxygen doesn't reach cells properly. That sort of things.
relaxation, good oxygen (maybe you can get O2 intake sessions), patience, and of course check for covid related data regarding lung damage (hopefully it's just temporary inflammation)
> i should add, anxiety level can influence this system a lot
The interesting thing is I have very low anxiety, I actually am taking this whole Covid thing in stride. I'm more of the "if it's my time, it's my time" sort of thinker. But when you stand up from a prone position and then world starts fading to black, it's not anxiety related!
I often forget this can even happen (it's not in the back of my mind), and when it happens again, I find it "extremely annoying", if you can believe that, rather than scary.
All the better then, I'm just passing info just in case. I had an extremely personal shock at the time and even if I tried to take things with calm and distance it probably influenced my system in various ways. It's subtle.
There is a subset of yoga that focuses solely on breathing called pranayama. I highly recommend it if you want to increase your lung capacity or build the muscles specific to breathing, and it has other benefits too.
Thanks, I knew the name but not it's purpose. I'll look into it tomorrow.
Beside the natural tricks, I'm also considering fasting, maybe cannabinoids (thx is said to trigger cell recycling in alveoli) and mayyybe tricks related to mitochondrial health (if doable outside medical facilities)
ps: even simple ground floor poses where your posture helps blood flow (head and heart at the same height) are super useful.
Not much sadly, it's actual cellular biology and above my skills tbh. It's part of the ideas floating in "longevity" websites and it seemed more interesting to try to monitor/help that part rather than fancier/newer ideas like epigenetic clocks etc. Mitochondria are good old established knowledge you know.. yet everywhere and important so why not investing some time to maintain that side ?
If i were in your shoes, I’d try to reach out to one of the groups researching long covid therapies. there is the beginnings of some research showing good results from existing drugs used for clotting disorders that may be easy for you to try under supervision. i’ll try to find some links when i’m back home later.
good luck, and i’m sorry for what you’re going through.
You could try John Hopkins, it’s a bit of a drive from NJ, but it should be doable. They have a whole team approach to dealing with long Covid and finding the right treatment for the individual.
You should consider that sequelae like this are characteristic of many forms of being very sick. It could be COVID specifically, but neither this article nor your experience establishes that causal link.
> neither this article nor your experience establishes that causal link.
Nor do they disprove it.
Someone that was healthy with no symptoms contracting a disease and, afterwards, displaying severe symptoms would, logically, require that the causal link be explored. It could have been a coincidence, but COVID is known to damage lungs and heart tissue.
My worry isn't so much that it's a coincidence, it's that stuff like that can be a function of basically any form of being _really sick_. Which would change around how one would think about the situation. Is it really COVID-19 that's the thing we want to point to here, or anything that could make you really sick (COVID included)? It really depends on what your goals are, but I think it's an important distinction.
Took me a little over 12 months to recover and feel back to normal. My heart still feels somewhat weird depending on the day, but my cardiologist told me that there's nothing to be concerned about and showed me proof that everything is working as expected.
Difficulty breathing, heart palpitations, dizziness, muscle twitches, and the brain fog throughout the last year has had its toll on my mental health.
Covid has brought upon one of the most depressive/anxious periods of my life. I don't know if it was because of Covid, the damage it caused along the way out, or if I had a huge panic/anxiety attack because of the symptoms.
Whatever it is, I have really been working on reducing stress, focusing on my mental health, and many of these symptoms have faded away and only return when I'm a bit on edge.
It has somewhat unlocked a superpower of knowing when to slow down at work, be in the present with my kids, and take a deep breath. I never had this ability before it.
I had an awful experience running for the first time after contracting COVID.. Unsure what strain I had but it was recent and I was careful so it's likely the "milder" omicron variant.
At the Gym, 3 weeks after testing positive the first time, I ran for 60s at 11km/h on the treadmill and my heart rate was 180bpm by the end.
For context, a 60s jog at that same speed prior to being afflicted would have resulted in a 130bpm heart rate.
Normally it would take running for 45 minutes to get to 180bpm..
But I got there (and felt awful) in 60s. I had to stop running.
Be careful returning to a full exercise schedule, esp after seeing effects like that. I see a running twitter group anecdotally observing a risk of a hard backlash of symptoms for runners trying to get back to their regular schedule too soon after even a mild covid bout.
Neat, I just recovered last week and was planning on a trial run this afternoon. Do you happen to have any links to the discussion in the twitter group?
Not my regular crowd, I fell into a thread last week and read through it, but can't find it now. There was a lot of side sniping from the sort of covid optimism denialist crowd - so they might have deleted parts of it and went to some other venue.
You also took time off training, it will take time to get back to your original form after that, could that account for any of it?
I think there is a psychological / confidence factor to running and if you're not meeting your target, it's easy to panic.
This happens to me when I run with other people, if they're faster than me, I often run slower because I panic that I can't keep up, which negatively effects my performance.
I don't do much running, mostly just weightlifting and a whole lot of walking but after I caught what I believe is the omicron variant relatively recently, I tried to go back to the gym and do a typical hard session. I felt like my heart/lungs were going to burst out of my chest after a heavy set that I normally might just be breathing mildy-heavy after.
I've definitely learned to take it a little easy for a while.
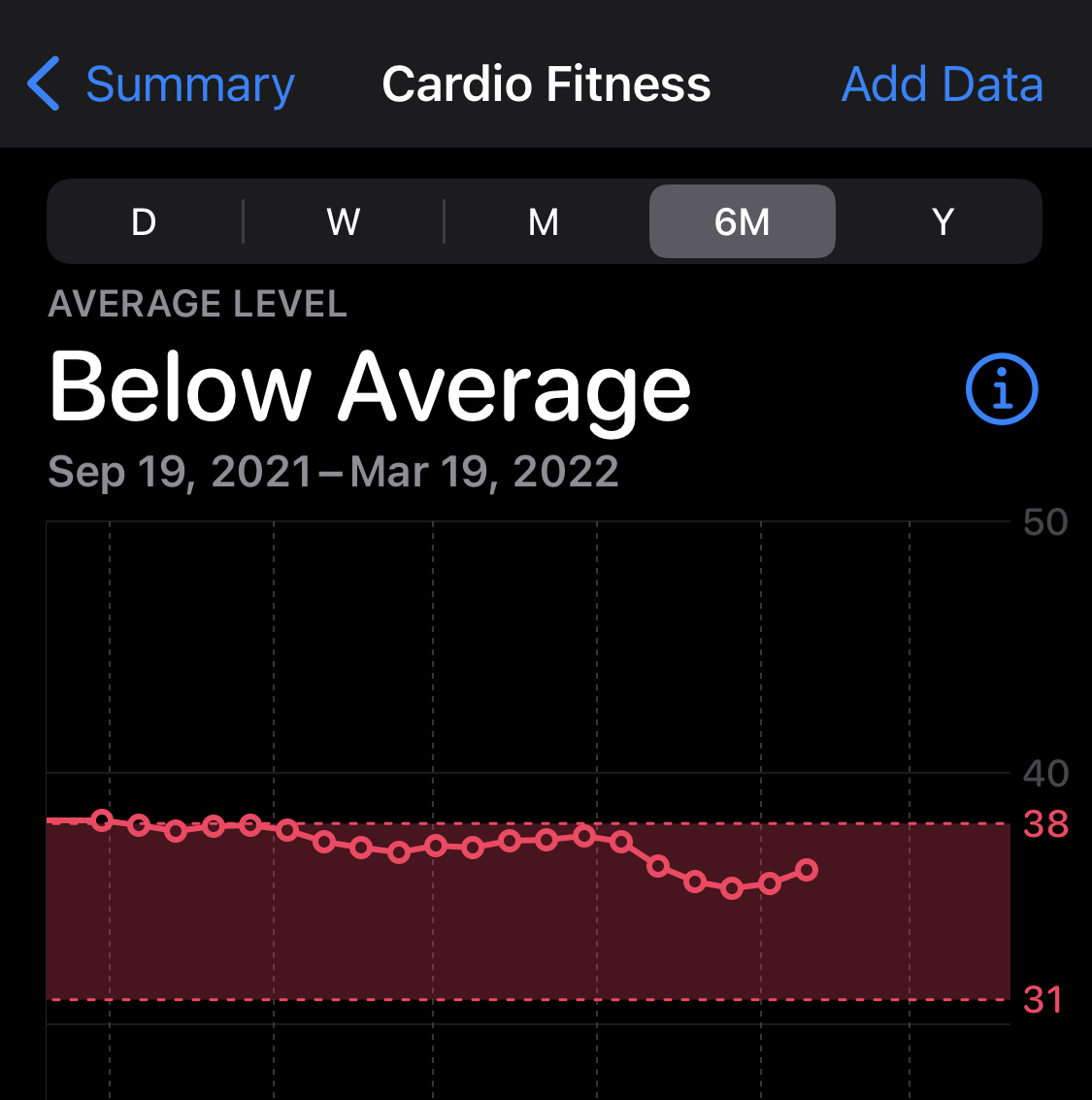
If anyone here has an Apple Watch and knows or suspects that they got COVID in the past year, open the Health app on your phone and look up your "v02 Max" figure on the Watch. This is a machine-learning guesstimate of how efficiently your lungs process oxygen.
(this was a huge letdown, back in September I had started a jumprope program in hopes of driving this number up, despite reading that v02-max is nearly hard-wired to a individual’s physiology)
Do you think you think it might be worth getting assessed by medical professionals before getting too disappointed ?
I have a Garmin watch and it does some pretty weird thing. My heart rate is super high apparently sometimes, it can tell me it's 180 during warmup when I'm hardly breaking a sweat, then go back down to 100 out of nowhere.
Maybe my heart is not working properly but I tend to think it's the "smart watch" doing funny things. The chest HRM seems more accurate but definitely not perfect because it relies on sweat for good conductivity.
Yeah, of course Apple and everyone else is always reminding us "this is not FDA-approved medical blah blah"
I'm aware that none of this is medical-grade, but every chance I get, I'll compare the data to actual clinical measurements and I've never seen anything more than a fraction of a percent off. Furthermore, the numbers from the Watch show clear trends; if the data was scattered or random, I would think that's "doing funny things." A clear change in data mere days after a COVID diagnosis… that's not a coincidence, c'mon.
My heart had wild palpitations for several days in the midst of having covid and post covid my resting heart rate is ~20bpm higher during the day and ~30 bpm higher during the night.
I had a very similar reaction that correlates to getting the vaccine. It took months for my resting heart rate to return to pre-vaccination levels. Maybe this means I would have died had I caught covid, maybe not, no way to know. It's scary how much this spike protein / immune response / etc seems to provoke adverse cardiovascular responses, even if there is full recovery in most of us.
I had already had covid 2x prior to general vaccine availability. I got totally owned in the short term but was back to working out pretty quick. The second Moderna shot completely wrecked me in a way having covid didn't, I had severe heart palps/skips for weeks. Sitting/standing at my desk and just having one after the other and would lose my breath between them. After that decided boosters could fuck off.
The vaccine is the safer controlled introduction to it in comparison to getting a full covid exposure. In a full covid case w/o being vaccinated would introduce more spike protein as well as a exposure to the sequences of the rest of the virus which could cause all sorts of other issues.
> It's scary how much this spike protein / immune response / etc seems to provoke adverse cardiovascular responses, even if there is full recovery in most of us.
Honestly I am wondering if this is sampling bias. Have we ever paid this much concentrated attention to a disease? When you consider what a virus does to the body, it seems likely that many other viruses that have been endemic for millennia have been wreaking pernicious havoc on our bodies and we just... shrugged it off.
Anyplace the body heals from a significant physical injury, there is a scar. It's never a perfect restoration. It seems almost intuitive that the damage from a virus would be similar, and there is documented evidence that COVID will attack neurons.
If you look at Fig1, describing the cohort selection, this study has two control groups. A historical as well as a contemporary control group. This gives an two different sample sources to reason about sampling bias. The data presented here are very likely not bias in the way your describing as it because of the contrast to both controls that would capture "it's always been that way" effect.
> If you look at Fig1, describing the cohort selection, this study has two control groups. A historical as well as a contemporary control group. This gives an two different sample sources to reason about sampling bias.
There's a clear difference in health between the cohorts.
Supplementary table 1 breaks down the cohorts and summarizes co-variates. Disturbingly, the COVID cohort is significantly fatter than the contemporary control group:
54% of the COVID cohort has BMI > 30, vs 42% of the contemporary controls, and 40% of the historical controls. They also have a higher percentage in long-term care (4% vs. 0.6%), a higher percentage with cancer (8% vs. 6%), chronic kidney disease (19.5% vs 16.7%), lung disease (15% vs. 11%), dementia (6% vs. 3%), diabetes (32% vs 22%) and hyperlipidemia (34% vs 25%).
The Covid cohort is basically a much sicker population, in almost every way. Re-weighting the populations doesn't correct for this disparity.
The authors have attempted to hide this by burying the data in the supplementary material, and presenting an "absolute standardized difference" that makes it look smaller than it is.
No that figure is the study being transparent on how it controlled for imbalances of selected input conditions showing raw numbers then the post processed reweighting of the samples. How does that fail as a way to account for differences in those conditions?
What would be your preferred technique of accounting for the differences of characteristics in those groups?
Look at supplementary figure 2. Their attempts to normalize the data do not eliminate the bias. The Covid-19 cohort is significantly sicker, even after adjustment.
This paper is discussing small differences in small numbers, and the single biggest difference between groups is the baseline level of health for the study participants. About the only thing you can say from this is that old, sick people are sicker after Covid-19 severe enough to put them in the hospital.
> The data presented here are very likely not bias in the way your describing as it because of the contrast to both controls that would capture "it's always been that way" effect.
That's not really what I said -- I'm not actually taking a stance on the conclusions of this paper. COVID has obviously been infecting massive numbers of people in the last couple of years, and if it is responsible for long-term cardiovascular sequelae as the paper concludes, of course it would be a more acute contributor over that period as compared to other historical causes simply by virtue of its pervasiveness.
Rather what I said is that the disease itself may not be causing "havoc" in the body at rates significantly different than other endemic viruses ("havoc" writ large: not only confined to cardiovascular sequelae, but among any long-term systemic harms). The bias that I am proposing is that we are _noticing_ these sequelae because A) so many people are getting sick at the same time, and B) because we are paying this much attention for the first time ever.
Like I just emphasized, they may not show up as statistically significant because
A) they are not pandemic, so the effect is of course much smaller
B) their impact is not necessarily primarily cardiovascular
Here's a non-exhaustive list of viruses with potentially overlooked sequelae.
Shingles (herpes zoster)
Rubella
Rotavirus
RSV
Norovirus
HPV
Hepatitis
Influenza
This is totally orthogonal to any possible defects in this study, which again I am not taking any stance on. It's merely a question of whether this study is anomalous for having been conducted in the first place. If we assume that the study is flawless, that means that COVID has long term health impacts -- fine -- but do we actually know if that's unusual for a virus?
I had heart palpitations randomly for over 8 months after Covid. I still find that my extremities tend to go to sleep and start tingling regardless of what I do (even them hanging by my side). It's extremely noticeable when I wake up from sleep. Even sleeping on my back with hands to the sides all night wakes up with them completely asleep and tingling, and other parts of the body seem to go to sleep easier than they did pre-Covid.
Thankfully, even though I likely had an early variant(Dec 2020), mine was not very extreme. I was constantly cold (like 45 minutes hot showers to get warm) and lost taste/smell, but I felt decent enough to run a 5k with it (probably stupidly, but at least it warmed me up), but the after effects have got me worried, especially the tingling in extremities which doesn't show any sign of going away.
I get the tinglies too since I've had covid. What helped me a bunch is making sure my shoulders are plenty warm. Often that involves a hot water bottle. Turned it from a nightly sleep interruption into pretty much a non-issue overnight for me, so it's worth experimenting with.
Huh, I got sick a few weeks ago and PCR test was negative for covid, but I had this same thing with the tingling arms last night, I woke up and it was my whole body pretty much, but especially bad in the arms. And now I'm getting it a bit in my feet / ankle area awake today.
I am having the same tingling issue where my hands fall asleep easily. Almost exactly as you describe. What could be causing this? I’m going to see a doctor in a couple weeks but wondering if I should try to see one sooner. Could it be caused by clots?
No clue. My doctor mentioned the possibility of nerve damage from covid but I moved before I could get in for those tests. Also check vitamin D and B12 (I was slightly deficient in B12, but even after supplements and other stuff it didn't change). Please let me know what you find out!
It helps some people. But there are people for whom it makes things worse. I know one of them. She had covid early in the spring of 2020 and made very slow progress to getting better. The vaccine put her back six months at least. I'm not saying someone should not get it, but find some statistics about the likelihood it will make you better vs worse.
Yes I'm vaccinated and boosted. It didn't really help. Got my second shot March 2021 (teacher), and symptoms didn't really go away until September, and I still have some as I said.
This is crazy but, I have had the exact same symptoms recently. At night, when laying on my stomach like I have slept my whole life, my hands start tingling like they are losing circulation. This is when flat beside my body.
any sort of decreased circulation can cause tingling. you may have had underlying cardiovascular/pulmonary issues for a long time, and are just now noticing it because covid.
I don't though. I went and got everything checked out after it started but before my insurance ran out (I moved countries and lost my work coverage). There was nothing on any of the tests that were run. And I've no other symptoms of anything really.
sure, it's hard to know without detailed investigation. i mention it only because i've personally had some underlying issues surface due to being unable to play basketball (my primary physical fitness activity) for over a year during covid.
After a bout of Covid and Moderna vaccines, I am now on a beta blocker, a Ca channel blocker and an ACE inhibitor along with a diuretic. I had never seen such high BP 180/140 in my arms. The virus and the S1 protein messed with my heart.
That sucks man :/ my anecdotal experience after having the original Covid strain and 3 full Moderna shots is that my heart is fine. BP is back to 105/60, resting heart rate is 50. I had long Covid for 8 months that fucked with my ability to workout and play tennis but now my stamina is fine.
So? The risk profile of vaccines has been researched to death as well as the effects of disease severity.
Part of doing science also means having looked at enough papers and conclusions to know which questions merit further research and which questions are of little relevance to public health. It is extremely unlikely that you'll find any surprises here, and considering the open questions of long covid and long-term health effects on the population on COVID, I'd much rather the focus be on the more important questions.
We don’t understand nearly enough about Covid, long Covid, or breakthrough cases to draw any conclusion about how much the vaccine mitigates the severity of long-term outcomes in breakthrough cases.
We have enough information to form an educated guess. But your attitude here is exactly why public health authorities have damaged their credibility and that of science itself in the past two years. They have repeatedly misrepresented their educated guesses as scientific fact - and then turned out to be wrong.
They're not "breakthrough" cases since the vaccine was never intended to stop transmission and very clearly does not stop transmission. They're just cases amongst people who took the vaccine.
> We found an increased transmission for unvaccinated individuals, and a reduced transmission for booster-vaccinated individuals, compared to fully vaccinated individuals.
And their definition of unvaccinated includes partially vaccinated (1-shot) and probably includes recovered individuals. See table 2 for their results which finds that boosters do significantly reduce transmissibility and susceptibility, but it is just very far from the perfect effect everyone would have hoped and wished for.
Vaccines are probably still more effective than masking in preventing transmission (given the average person's adherence to masking guidelines) and the effect would intuitively (to me anyway) seem likely to stack.
> But your attitude here is exactly why public health authorities have damaged their credibility and that of science itself in the past two years. They have repeatedly misrepresented their educated guesses as scientific fact - and then turned out to be wrong.
Where has that happened for this? Every study that has shown disease severity correlated with vaccine usage has shown the same results, over and over, for each variant: vaccination correlates with symptomatic disease severity which correlates linearly with long-term effects, in every observed metric.
This has appeared again and again and again in dozens of studies, to the point where it is the null hypothesis; you'd need to make a real case with novel, contradictory evidence to show that this is not the case.
In every domain of medicine there is some degree of guessing and basing off of historical data for a cohort; you can't test every patient for every possible thing that could ever affect them. Instead you pick and choose the most significant factors and use that as your guidelines. Research efforts for COVID are very large, but also limited; there is no evidence to contradict this and it's not worth researching.
If you actually kept up with domain experts during the pandemic, you'll see that there were many open questions over which they kept interest, and many open questions where they did not care much. The reason for that has to do with the acquired knowledge of having studied hundreds of other diseases and similar cases; they tell you how to explore the domain, seeing where things are likely to be different, and where they are not.
Overall a skim makes this seem like a good effort to me and potentially informative. However, I want people to understand a couple things:
1) This article is not an experiment and doesn't establish that COVID-19 is the causative agent here. They do a variety of statistical tricks to get a little closer to causality. I am particularly worried about this part:
"To adjust for the difference in baseline characteristics ... variables were selected based on prior knowledge1,7,24,25. The pre-defined covariates included age, race (White, Black and Other), sex, ADI, body mass index, smoking status (current, former and never) and healthcare use parameters, including the use number of outpatient and inpatient encounters and use of long-term care. We additionally specified..."
That's nice, but it involves a lot of experimenter degrees of freedom and doesn't control for the main thing that strikes me as relevant here: behavior. It's not like people were randomly selected to get COVID or not, they were getting COVID or not largely as a function of their behavior. People who are more risk-tolerant and / or less norm-compliant are going to have different health outcomes.
EDIT: point 2 is wrong, I misread the data
2) The effects aren't large. For individual cardio conditions, max 1% increase. Overall, max 5% (many of which aren't serious).
EDIT: begin the part I still believe again:
I'd like to see an analysis that looks at these outcomes merely on the basis of care setting. I.e., if you end up in the ICU for anything at all, how does your increased risk of $CARDIO_PROBLEM change relative to COVID specifically?
It's fun to talk anecdotes, but the data isn't ever as exciting as people would like to believe. I think it's very important to work against the hype machine because that's the only way we'll build real evidence-based progress.
I'm reading the graphs in the results section with the hazard ratios. All hazard ratios are above 1.5, which if I understand hazard ratio correctly means at least a 50% higher risk compared to regular population?
Am I misunderstanding hazard ratios? Or do you get the stats from elsewhere in the paper?
It’s interesting to see less obese and younger people more affected. Maybe it’s either because of vaccine status that another commenter asked for, or more deaths in those cohorts.
I got Covid in December and it took me roughly around 2~3 weeks to recover. Basically my symptoms were on the light side (minor cough and lots of phlegm. Luckily I didn't have a fever but on the worst day I had a headache and fatigue. Most of the recovery period, I was just resting and not really doing any intense physical activities.
It was only in January that I started running or exercising intensely and noticed only a slight decrease in performance. Mainly that was due to not exercising for a month or so. However, overall I didn't notice that running/working out was significantly (>10%) harder but In my case, I took a very longer break than other. Just some food for thought
i also had a recent bout, probably omicron. 2 days of fever and fatigue, and then a couple days of light coughing to get all the resultant phlegm out.
the kicker is that i feel better afterwards, due to the fever (i'm guessing) also clearing out a lingering cardiopulmonary issue (perhaps from a pneumonia bout a few years prior) that had gotten progressively worse during lockdowns (when gyms were closed for months).
Aside from the study being interesting topic, I love the inclusion of Fig 1 the cohort construction diagram. I wish more papers would include that as a standard item.
Can anyone explain the findings? A quick google of 'excess burden' term didn't yield a clear definition, there is a similar term in taxation, but that seems unrelated.
I believe that 'excess burden' is essentially how many more people than expected would show these outcomes. IE, if normally you'd expect to see 5/1000 people in a control group experience a stroke, but observe stokes in 15/1000 people in your non-control group, the excess burden would be 10/1000.
HR appears to be 'hazard ratio' which is simply a ratio between the two groups. The above example would have a hazard ratio of 3, as three times as many people presented with the outcome than expected.
The meat of this seems to be in confirming that if you're not hospitalized the long-term effects are minimal. Not _zero_, but very small.
The abstract states that "These risks and burdens were evident even among individuals who were not hospitalized during the acute phase of the infection", but I'd urge attention to the data as this implies only that there is a detectable change, it's not a judgement on the size of the risk.
The worst cases are in intubated patients that basically lost proper oxygen flow for extended periods of time.
I'd guess you're being downvoted because the article describes a different conclusion:
"[long term] risks and burdens were evident even among individuals who were not hospitalized during the acute phase of the infection."
Though it does seem to make a distinction in grade ("these risks increased in a graded fashion according to the care setting during the acute phase (non-hospitalized, hospitalized and admitted to intensive care)"), it doesn't seem to support the idea that the impacts are limited to the hospitalized.
Yes, it's evident in the scientific sense of the word - the risks exist.
They're just very small. If you look at the data, the risk ratios are in the range of 1.0x-2.0x, on outcomes which in healthy individuals are extremely rare to begin with. Same with the excess figures.
The logical conclusion given the rest of the data is that these outcomes would be concentrated in those who were very ill but below the threshold of hospitalization.
The study itself doesn't bin the groups far enough to show the implication for the asymptomatic or those with very minor symptoms, but there's a clear exponential trend that associates acute severity with long-term severity supra-linearly.
You have moved the goalposts from "not hospitalized" to "asymptomatic or very minor symptoms". About half the people I know who got covid (and knew about it) had, or are currently having, a very unpleasant time.
> You have moved the goalposts from "not hospitalized" to "asymptomatic or very minor symptoms". About half the people I know who got covid (and knew about it) had, or are currently having, a very unpleasant time.
And 100% of the people I know who had it (measured in the tens; including myself) have had no lingering symptoms at all.
Anecdotes are not science. It is not "moving the goalposts" to note that lingering symptoms correlate with severity. The authors of the paper have already shown this, but didn't break it down enough.
The study itself states that in patients that are not hospitalized the risks of various heart conditions increase on average by ~1.5-2x.
That's for the entire cohort of non-hospitalized individuals, it's an average.
If you assume that they're uniformly distributed (e.g. if you assume that the relative risk of future myocarditis is identical for someone who has no symptoms, and for someone who's bedridden for a week with breathing difficulties but non-hospitalized), the figures show that if you're not hospitalized your risk of myocarditis and other heart issues is multiplied by about 2.
If the study were binned more finely I think you'd see a 5x multiplier if you have mild illness (mild in the clinical sense which simply means non-hospitalized but exhibiting symptoms) or no discernable effect if asymptomatic. I agree that there is no specific data for this, I'm extrapolating the curve.
> About half the people I know who got covid (and knew about it) had, or are currently having, a very unpleasant time.
We're not debating this point, this is a paper showing the correlation between the short term and long term effects of the disease.
You say "only" a doubling of the risk of rare heart related issues, over the course of a single year. I say gee, it sure sounds like the virus massively fucked with their system. Large statistical anomalies are measurable an entire year later. Whether the baseline risk of such issues is high or low is irrelevant, since the main takeaway is that everyone basically gets Long Covid, to a greater or lesser extent. Remember that this isn't the only measurable effect either - it's just the one this paper is talking about, and it fits into a wider pattern of research indicating systemic damage even in so-called "minor" cases.
Again, speaking from both personal anecdata and the wider scientific consensus - if you have symptomatic covid, it takes you a long time to feel "normal" again.
The data doesn't imply that ~everyone has long term effects because we don't know the distribution in the non-hospitalized cases.
> if you have symptomatic covid, it takes you a long time to feel "normal" again.
The non-hospitalized group in this study includes both symptomatic and asymptomatic.
This comment thread is a bit weird, you seem to be attacking me on an emotional basis. I'm interested because I think this data shows a good correlation between severity of disease and severity of long term prognosis, that's all.
I have an interest in knowing this, as we all do, because like basically everyone else, I've had coronavirus, and if the data shows that this now means I have an elevated risk of heart issues I should be careful with things like heavy exercise. I don't think it does based on the correlation shown (I didn't have severe coronavirus), so it's actionable information.
If you disagree with my assessment that a 2x multiplier on a rare event is not worrisome, that's fine - that's just like, my opinion, man. :)
> This comment thread is a bit weird, you seem to be attacking me on an emotional basis. I'm interested because I think this data shows a good correlation between severity of disease and severity of long term prognosis, that's all.
Your original comment reads as a much stronger statement:
> The meat of this seems to be in confirming that if you're not hospitalized the long-term effects are minimal. Not _zero_, but very small.
I think also 'the long-term effects are minimal' reads too broad since this study only covers a narrow set of long-term effects while your original comment can read as applying to all long-term effects.
> If you disagree with my assessment that a 2x multiplier on a rare event is not worrisome, that's fine - that's just like, my opinion, man. :)
I would want to look at the number of people effected a year before and after the change in order decide if it was worrisome or not.
> Large statistical anomalies are measurable an entire year later.
Doubling of a very small number is not a "large statistical anomaly". Figure 5 shows that the difference is skewed strongly toward the hospitalized, and that the largest difference observed for the non-hospitalized cohort is measured at maybe 10 per 1,000 (1%) and most well-below that (single-digit difference per 1,000).
This means that expressing changes in a tiny value relative to its baseline (e.g. "3x as likely") sounds more impactful than expressing the same changes in absolute terms (e.g. "from 0.01% to 0.03%").
Individually maybe small (I actually am not sure 1-2x seem like a minimization of the impact but I'd leave it to further reading and discussion to settle that), but in a public health sense it might mean a doubling of cardio treatment resources in a system where growing those resources is not a fast response and could have follow on effects on quality and availability of treatments.
The article isn't about the risks of vaccination but of covid infection. The only mention of vaccines is in a section where it discusses controlling for vaccination status and concludes that the risk of myocarditis from infection is present even in the unvaccinated.
One thing I've wondered about with issues from vaccine side effects is if they are in any way related to how the body would respond if the actual disease was contracted.
This is not to discount the effects or concerns about it -- just curiosity.
Knowing that this is clearly off topic here, one thing that crossed my mind wrt myocarditis amongst the vaccinated is this: amongst athletes, myocarditis is clearly linked to exercising (or even competing) while dealing with an infection (not limited to Covid19 at all, other than that this one seems to be particularly nasty). The risk of inflammation rises when when athletic stress and infection stress (or immune reaction stress, apparently) coincide. This is common knowledge amongst athletes, most would have taken a break from training even if no doctor ever mentioned it.
But we do seem to see an uptick not only amongst the infected but also amongst the vaccinated (note: I do believe that infection is much worse, but vaccinated to infected are roughly 80:20, so it tends to look kind of even). What if the risk of myocarditis was not so much caused by coincidence of training intensity and immune stress but also by coincidence of immune stress and whatever happens during training recovery (when the body does the actual work of adaption, you don't get better during training, you get better afterwards)? When you tell an athlete that they get their shot on Wednesday and they should better take some rest days afterwards, it's as predictable as Wham in December that they will throw in some serious training load on Tuesday. Chances are they'll train extra hard so that they need those rest days anyways. (for me it was Sunday/Monday)
Now the thing I find particularly interesting about this speculation: if this mechanism was real, myocarditis risk not from high training load coinciding with immune stress but/also from immune stress coinciding with post-load recovery, it would be highly unlikely that we'd know about it. Because with naturally occurring immune stress, we don't ever have a clearly defined point in time when it started, and we certainly wouldn't ever deliberately schedule it so that we could arrange for training load to happen right before.
About 105 vaccine recipients reported at least one AEFI symptoms following COVID-19 vaccination (incidence proportion 6.4%, 95% CI: 5.3%, 7.7%). All AEFI reported were minor which were managed by tablet paracetamol and subsided after 1–2 days. Fever (65, 3.98%) was the most commonly reported AEFI followed by myalgia (54, 3.30%) (Fig. 1). About 48 (2.94%) study participants reported 2 or more AEFI, most common being fever with myalgia (19, 1.16%) and fever with headache (18, 1.10%). No severe or serious AEFI was reported among vaccine recipients.
I think adverse just means "not good" as one could also see neutral or even positive effects; one would say severe or serious (as in the text you quoted) as strength modifiers if applicable, but the word "adverse" shouldn't inherently make something sound strong or ever feel synonymous with "serious".
Yeah, I wish we had some research about this. Somehow everybody on internet believes that covid will be always, literally always worse than vaccine side effects.
It is objectively pretty much always the case, this has been studied to death. /r/covid19 has dozens of studies from all over the world quantifying the risks of heart disease for all vaccines, all age cohorts, and vaccination statuses.
The comment misrepresents the content of the article in a way that's trivial to see if you simply read a few paragraphs of it (it's about the effects of infection, not vaccines). The flagging is merited.
With the supposed cardiovascular and brain dangers of COVID, I have still been working pretty hard to avoid infection, which is definitely getting to be old news. My apartment isn't that nice.
Glad to see some science putting numbers on what the odds we're all against in terms of long-term damage.
Same, my wife and I have been more or less holed up the past month or so, waiting for our area's death rates and hospitalizations to normalize, but honestly I'd like even the case count to drop more before I venture back into the world.
Yes, I could get COVID and yes, I'd probably be fine, but the more information coming out around lingering effects give me serious pause about the "everyone will get it eventually" route.
I'd rather never get it, if that's possible, and honestly if the numbers continue to drop as they have been, I'm a few weeks away from that being actually possible in my area again.
The virus will never disappear. Regardless of your area's death rates, you will be exposed eventually (unless you spend the rest of your life quarantined).
Yes, but eventually is not today, and
a) there may be a better treatment for long COVID by then,
b) hospitals in my area will hopefully be less overwhelmed,
c) vaccinated, healthy people can still die to COVID-19 and,
d) maybe I can skip Omicron and get some other, even less severe, variant instead.
The trendline is heading towards Fall 2021 levels, which weren't great but still at my personal acceptable levels of risk. A few more weeks, hopefully.
After a decade of lifting heavy stuff, at the beginning of COVID I switched from powerlifting to running. I don't feel as powerful and definitely have lost some muscle mass, but I'm down 35 lbs and my resting heart rate sits in the 40's now. Fitness is absolutely what you make of it.
Not everyone want to run with mask around dirty city block.
It is really interesting to see this mental gymnastics, if someone is fat, gets virus and dies, it is "the plague". But here we have dozen people talking about "personal responsibility".
a) Never seen a single city mandate masks for exercising outside. Especially since it’s quite dangerous to limit your oxygen flow. So you should have been fine to run outside.
b) Some of the toughest workouts I’ve done were inside. You need to stop being so close minded.
Mask is needed for the smog, that is why I want to run indoors at gym on threadmill. It also shields me from aggressive drivers and traffic.
Masks do not restrict oxygen flow, there are several studies to prove it! It is perfectly safe to wear double mask for entire day at work or at school!
I also like to do tough workouts inside, at gym! I do not have gear or space at home.
I did a lot of stationary exercises using my own body weight to keep up my level of fitness. Nintendo's Ring Fit, Apple's Fitness+, even YouTube, there are so many avenues to explore.
The other commenters are right in saying that there are excuses, and you seem to be full of them.
That would be truly impressive if less than 2 years of occasional closed gyms turned you from perfectly healthy to at risk of a heart attack. You've managed to squeeze a lifetime of bad choices into two years.
I agree about the gym - you can’t replace it at home unless you’re seriously rich, like many tens of millions of net worth. My gym has pools, lots of heavy weights, many odds and ends and equipment you’d never buy.
I can get a vastly better workout there than by doing pushups at home.
For various reasons, I don’t run, which leaves cycling and swimming for cardio. I also like to lift heavy - this means a large variety and quantity of weight. I need a gym.
{kind=link}
Even things like climbing stairs has become a chore. One top of that, I was experiencing syncope on standing which they sent me to a cardiologist for. I couldn't complete the treadmill test to anyone's satisfaction so now we have to explore this further.
None of this existed prior to getting Covid, and it's far past the point of "it's all in my head". With the fainting on standing, I would literally drop to my knees as the world faded to black. I've never experienced anything like that in my life.
The shortness of breath is just another one to add to a list of problems now.
Note I was double-vaxxed when I caught Covid. I'll have to assume Omnicron although I have no actual data on that. It was a breakthrough case and I had a 104 fever, cough, and shortness of breath (that's why they admitted me). It's been downhill since then.