If you're 80 years old, you probably should not receive a subsidized hip replacement.
If you can't afford it on your own, there should just be a palliative care mandate after some age. We shouldn't save the soon-to-be-dead at the expense of the people with a long time horizon.
Or, we should pay doctors far less. I don't think they're multi-millionaires in other countries. Not all of them are in America, but many of them are.
> If you go to a hospital in the United States, it's a lot of old people getting expensive care.
You think hospitals aren't full of old people getting care in other countries? And do you think it's possible that young people in the US don't go to the hospital because they can't afford to?
I took that out because I didn't think it was relevant. And yes, that is my point. Young people can't afford insurance in America. It's terrible. I think the GLP-1s are going to make things better. A huge problem, as everybody knows in America, is obesity. That's also a major tax on the system.
The government subsidizes a portion of ACA payments depending on income in America. Without the subsidies, it's unaffordable for probably 95% of the population. That's why most people rely on employer-sponsored healthcare.
What other choice is there? About 10% of all US healthcare spending is on end-of-life care [1]. It's not pleasant to talk about, but it is a discussion that needs to take place.
Speaking only of the financial aspect, not any other ethical issues:
Those end-of-life patients paid into the system, earlier in their lives, financing the cost of earlier generations of end-of-life patients. It would be unfair to change the social contract now.
In my opinion, it is no different from how adult taxpayers finance public education for children. It is a rolling responsibility from generation to generation.
You may be able to alleviate this financial issue (and not any other ethical issues) by phasing-in this policy change with the youngest generation of Medicare taxpayers, somehow.
> Those end-of-life patients were paying into the system, earlier in their lives, financing of the cost of earlier generations of end-of-life patients. It would be unfair to change the social contract now.
> In my opinion, it is no different from how adult taxpayers finance public education for children. It is a rolling responsibility from generation to generation.
This hits upon the core issue: the next generation is substantially smaller than the last and relative costs have ballooned due to greater availability of therapies. The generational contract is that you pay your taxes a percentage of wages -- in effect, a PAYG mechanism. If wages do not rise sufficiently to cover increased costs, that does not imply that the generational contract was unfulfilled; the taxes were paid.
The demographic pyramid and weaker than necessary wage growth really renders the care demanded burdensome to the point where we have already provided elderly cost advantages in insurance in the form of cost premium multiple maximums and medicare from payroll taxes while beggaring the rest of the population in the process.
> In my opinion, it is no different from how adult taxpayers finance public education for children. It is a rolling responsibility from generation to generation.
Fundamentally, children are an investment. They produce cash flow (taxes) from increased public health. The end-of-life are not; by definition, they will be dead soon. It's a horrible thing to say, but in the face of ever increasing elder care burdens and weak public debt/gdp ratios, what real choice is there?
> If wages do not rise sufficiently to cover increased costs, that does not imply that the generational contract was unfulfilled; the taxes were paid.
That's an interesting alternative view I had not considered. I think it is debatable. I believed the generational contract to be "healthcare for 65+ with 20% copay, etc., no gov. expense spared" whereas you argue the generational contract to be "Medicare payroll tax of X% is constant over all time; spend it wisely." I would argue the first option was the original intent of the Medicare law.
> Fundamentally, children are an investment. They produce cash flow (taxes) from increased public health. The end-of-life are not
You could argue the same for the end-of-life, in at least two ways:
* the end-of-life patient has already produced cash flow to the government, just in reverse order from the student
* Good education produces a higher taxpaying adult, the investment you refer to. I would argue the assurance of end-of-life healthcare also produces a higher taxpaying adult.
I acknowledge the costs have gone up faster than wages+population.
> I believed the generational contract to be "healthcare for 65+ with 20% copay, etc., no gov. expense spared" whereas you argue the generational contract to be "Medicare payroll tax of X% is constant over all time; spend it wisely." I would argue the first option was the original intent of the Medicare law.
I appreciate this view, but it is ahistorical and does not reflect the history of Medicare law.Taken from [1]:
> By the late 1970's, the growing expenditure trends and the changing demographics (an increasing proportion of the U.S. population 65 years of age or over) combined to endanger the solvency of the Medicare Trust Fund. The rapid increases in expenditures for the Medicare program, as well as health care services in general, constrained the ability of the Federal Government to fund other health and social programs. To a certain extent, the growth in expenditures also endangered the Nation's overall economic productivity.
> At the same time as health care expenditures were escalating, some say uncontrollably, the political landscape began to change dramatically. The national mood brought calls for fewer taxes, for reduction of budgets, and for deregulation of market sectors, such as transportation and health. This conviction of less general involvement by Government was reinforced by mounting public pressures surrounding growing budget deficits; Medicare, like other Federal programs, increasingly competed with more global policy objectives. In the space of a few years, the Nation moved from an era when health care was considered a right for all citizens to an era when cost considerations became the dominant issue.
And bear in mind, this was just ~10 years after Medicare was introduced. The nation has always prioritized the future over the past, and has either reduced or restructured benefits to ensure a healthy economy ahead of Medicare.
> You could argue the same for the end-of-life, in at least two ways: * the end-of-life patient has already produced cash flow to the government, just in reverse order from the student * Good education produces a higher taxpaying adult, the investment you refer to. I would argue the assurance of end-of-life healthcare also produces a higher taxpaying adult.
This lacks an understanding of Medicare. Medicare is fundamentally a PAYG mechanism; the trust fund was a short term surplus which is slated to be depleted by 2033 [2]: a mere 8 years from now. Part of this occurs due to poor investment strategy (treasuries only, effectively) but the biggest contributing part of this was the demographic boom. The time for "more cash flow to save for Medicare" isn't today it was 30 years ago. A failure to raise taxes 30 years ago should not constitute an obligation on the youth of today and placing the burden of an excessive tax because of poor demography and unwillingness of prior generations to raise taxes on themselves only harms economic growth at the expense of the elderly.
That's a reasonable question with several answers.
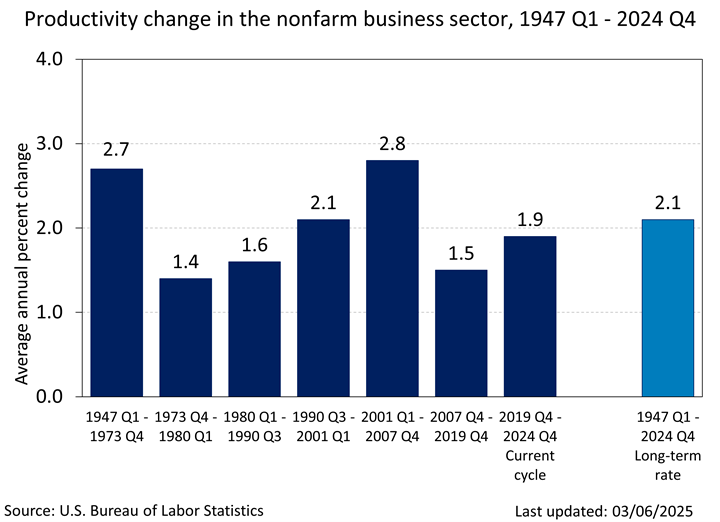
One is that US healthcare cost inflation is very high. The average family premium in 1999 was $6k, it is now $27k, for an annual cost increase of 6.1% per year. The long term rate of productivity increase is much lower than that, at only 2.1% per year.
So costs have just risen a lot more than productivity has.
Another reason is that productivity increases aren't evenly distributed. Most productivity growth has been in other sectors, primarily oil+gas and tech i.e. sectors dominated by men who aggressively automate. Healthcare has seen no increase in worker productivity for decades:
Output is up, but only because of more hours worked. And much of that output is growth of administrative overhead, not actual healthcare as most people perceive it.
Soaring demand + zero productivity growth + cost inflation 3x higher than inflation + no political will to control costs = a death spiral in which the lowest risk decide to go it alone and drop out, leaving ever higher premiums for the rest.
And productivity in society has gone up by huge amounts since the 1960s. Just since the 90s it's more than doubled, but going back to the 1960s it's much more than that. So you can't just say 'but population dropped'.
Fundamentally what is the purpose of society if the improvements it makes over time don't improve its's citizens lives? If even with tripling it's economic output it can't care for it's people (just because they are old doesn't make people not part of society)?
This argument is a moral event horizon and the problem should be resolved by other means.
Once one decides to ration healthcare based on estimated remaining QALY, the same logic says we shouldn’t subsidize, e.g., healthcare for people who suffer from cystic fibrosis, or HIV, or aggressive cancers, or. . .
Or if you’d rather, there are millions of children without healthcare in the United states. Would you forgo your access to healthcare for them?
> $365 billion of it went for end-of-life care. [1]
That’s all? Musk alone is worth twice that, and who knows how many QALYs he has left but it can’t be that many. He seems pretty miserable most of the time.
> Once one decides to ration healthcare based on estimated remaining QALY, the same logic says we shouldn’t subsidize, e.g., healthcare for people who suffer from cystic fibrosis, or HIV, or aggressive cancers, or. . .
Those are risks. Risks are insurable. However, death is a certainty. It is very reasonable to discuss what we believe society should subsidize for end-of-life care as it will impact everybody, myself included.
> Or if you’d rather, there are millions of children without healthcare in the United states. Would you forgo your access to healthcare for them?
I don't see what pediatrics has to do with end-of-life care in the context we are discussing (Medicare), but I would much rather subsidize pediatrics than elder care.
> That’s all? Musk alone is worth twice that, and who knows how many QALYs he has left but it can’t be that many. He seems pretty miserable most of the time.
Musk is worth 244B [1]. Even if we could tax wealth 100% into cash, we would fully exhaust the wealth of the 25 wealthiest American families within 7 years. These expenses, however, will likely continue for the next ~20 years. We need to discuss benefit cuts or tax hikes on the American population writ large.
> Once one decides to ration healthcare based on estimated remaining QALY, the same logic says we shouldn’t subsidize, e.g., healthcare for people who suffer from cystic fibrosis, or HIV, or aggressive cancers, or. . .
Not everybody gets cystic fibrosis, or HIV, or aggressive cancers. These are a risk. That is fundamentally an insurable risk. However, we will all die. No matter how much money is spent, death comes for us all in old age. Discussing how much is an appropriate cost for end-of-life care when aged is very much a societal question.
> Or if you’d rather, there are millions of children without healthcare in the United states. Would you forgo your access to healthcare for them?
This remains a question, even in Europe. See [1] for a discussion as early as 2000 regarding rationing in the NHS.
> That’s all? Musk alone is worth twice that, and who knows how many QALYs he has left but it can’t be that many. He seems pretty miserable most of the time.
That is a cost each year, and Musk is currently at 244B [2]. We have roughly 20 years of this level of spending or greater. Even if we assumed we could tax Musk 100% (which isn't practically possible because who liquidates his positions), where do you propose to acquire that level of ongoing cashflow? Within 7 years, we would fully exhaust the wealth of the 25 wealthiest American families, even at 100% tax rate. End-of-life care is mind-bogglingly expensive for the United States economy. This either needs to be a tax hike which realistically will it everybody or a benefits cut.
I'm middle-aged so I don't really have a long time horizon but I do have expensive insurance. If you have employer-covered insurance, you don't know what the hell you're talking about. So it's easy for you to say.
The hip seems like such a bad example to me. First of all, who do you think needs hip replacements? It's not young people; surgeons don't even like to do them on young people (and to a joint replacement surgeon, "young" is under 60) since there's a good chance they'll outlive the joint itself. And it's a one-time cost for a surgery that increases an old person's independence vs an ongoing cost of palliative care (whatever that means) and having to provide more care for someone who has a potentially treatable disability. Hip replacement is considered "the surgery of the century" - the 20th century that is, because it is one of the most successful in terms of function and satisfaction provided to patients.
>Perhaps we could just have a 'poor people incinerator' for those whose expected medical expenses exceed their net worth?
Thanks for putting that out there. Give it 10 years, and I'm thinking we'll see the first "bio-repurposing vats". Never mention crap like that on HN. Too many closet psychopaths looking for a big break.
Understand the attempt at shaming. But there are likely a non-trivial number of readers here with such Methuselan inclinations.
I mean you called to just let 80 year olds die. If they can't care for themselves, can't move around, and are left in constant pain, they end up just dieing.
Then you gave the wisdom 'older people use more medical care than younger people'. Like yeah, that is how life/the universe works. My old car requires more maintenance then when it was new. But funny thing about young people, they too will one day be the old person.
No, I said palliative care. That's to ease suffering. So you're telling me we should forego cancer treatments for young cancer patients so 80-year-olds can get hip replacements? Is that what you think? Are you crazy? I never said just let people die. That's insane. It's about cost. In America, they don't just give healthcare for free, like wherever you probably live. I wish they did.
You may not have realized it but leaving an 80 year old bedridden and unable to care for themselves is a death sentence. Any doctor sending an 80 year old home with a shattered hip and not a replacement knows that.
I live in red state America, like one of the super red states. The American healthcare system decided it didn't make sense financially for our small community to have ambulance coverage. You know what we in red state America did? We taxed ourselves and have much better ambulance coverage/care then we ever had before.
Nobody can ever imagine a better system, even if it’s used in literally every advanced nation in the world. Nope, instead we have to let Grandpa die painfully to keep those stock prices up.
I’m starting to think Capitalism as it’s practiced here is a death cult of some kind.
The better system that the rest of the world uses is letting grandpa have a bad hip. Absolutely insane that you take a huge part of what makes other systems cheaper and claim other systems would never do that and capitalism is to blame for everything bad.
Well, I mentioned palliative care, but in general, I agree with you.
I would much rather doctors just get paid less. I took my son to the ER. He had a very high fever. They gave him a child's aspirin and me a $700 bill.
I just don't know what the answer is. And really, if you go into a hospital, you get the sense that there's people basically taking advantage of subsidized health insurance providers and patients both. Health insurance in America is absolutely atrocious. Next to gun fanatics, it's the worst thing about this country.
Because the instruction from most pediatricians is to send kids with persistent (not responsive to acetaminophen and/or ice bath) fever above 104F to the ER, especially after hours. Very, very rarely will you find a pediatrician available outside an ER setting after hours.
Something changed in the US in the last 15 or so years that caused our whole country to become a death cult. All I see in the economics is a bunch of looting and pillaging before the music stops
The rest of the world mostly also uses subsidized private healthcare (except for the UK, where healthcare is far worse than in the US).
The US system works well if you can pay the bills. It doesn't have the undercapacity issues the UK has, for example. The unique problem is costs. Controlling costs would mean consumers strongly supporting aggressive action by insurers if they take actions to push costs down. What Americans do is the opposite: they stage protests and demand immediate political retaliation on insurers who try to control costs. Then left wing politicians condemn the insurers, and they fold in the face of public pressure. Medical staff know the public acts this way and so bends insurers over the barrel, knowing people will blame the "capitalists" (who have tiny margins) over the frontline doctors and nurses who are actually taking the money.
In other countries the public doesn't act this way and costs are more reasonable. Sometimes insurance premiums even fall. Switzerland has a two tier system with basic mandatory health insurance that's basically controlled by the government (private firms provide it but there are price controls and they can't refuse customers). And it has supplementary insurance for higher quality care that's almost free market. This year basic premiums went up 5% and supplemental premiums fell 0.9%
{kind=link}
If you can't afford it on your own, there should just be a palliative care mandate after some age. We shouldn't save the soon-to-be-dead at the expense of the people with a long time horizon.
Or, we should pay doctors far less. I don't think they're multi-millionaires in other countries. Not all of them are in America, but many of them are.